Hallux Rigidus - Cheilectomy
What is a Cheilectomy?
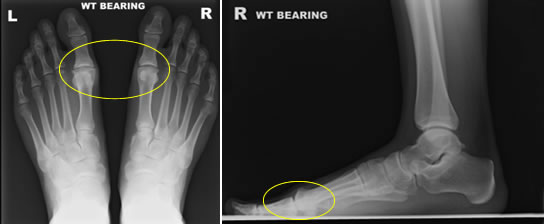
A Cheilectomy means you remove the build up of bone on the top of the 1st MTP joint. It is derived from the Greek word “Cheilos” meaning “lip”, and you literally remove a lip of excessive bone from the joint. The operation can be done via a very small open incision or alternatively via a minimally-invasive approach with keyhole incisions. You can discuss this with your surgeon before surgery.
What is it for?
The operation is designed to treat Hallux Rigidus or mild arthritic changes in the joint. It does not involve replacing or fusing the joint. It is best to think of it as a “tidying up” procedure in the big toe and to increase the joint movement. The good thing about this operation is it works fantastically well in the majority of suitable patients.
How the surgery is carried out
It is a day-case procedure. The operation is done under a general anaesthesia and an added injection in the foot to numb it for after surgery. The operation itself can be done via keyhole incisions or alternatively via a single 2cm incision over the top of the big toe. The procedure involves excision of the build up of bone that is mechanically blocking the joint to allow normal movement afterwards. Dissolvable skin stitches are used.
What to expect immediately afterwards
Your foot will be bandaged, numb and pain free. You will see a physiotherapist who will advise on toe movements and walking in a padded stiff shoe supplied. You will be discharged only when comfortable with an appointment and pain-killers as required.
Recovery in the first few weeks after surgery
- Elevate your foot as often and as much as possible to reduce swelling.
- Mobilise as instructed, but only for necessity indoors and outdoors.
- Some blood ooze can be expected in the bandage, if worried contact the Consultants clinic.
- Anti-inflammatory medications such as Ibuprofen or Voltarol can help.
- After 1 week move toe up and down for 5 minutes four times daily. The wound dressing can stay on the toe but you can remove the bandaging. The physiotherapist will show you this before you are discharged.
Post-operative clinic schedule
- 2 weeks - Wound check
- 6 weeks - Clinical review
- 12 weeks - Clinical review and discharge
When can I start to walk?
- 0-2 weeks - Full weight-bear in hospital shoe
- 2-6 weeks - Full weight-bear in own wide shoe/hospital shoe
- > 6 weeks - Full weight-bear in normal shoes
How do I wash and shower?
In the first 2 weeks keep the bandaging/foot totally dry. You may shower with a waterproof cover over the foot. After 2 weeks you can only shower if the wound is healed but gently dab the wound dry.
How can I look after the wound?
Once out of bandaging, do not pull at scabs but let them fall away naturally. If your wound becomes red, swollen or sore you need to see your Consultant to ensure there is no infection present. Your physiotherapist may advise on wound massage.
Physiotherapy and Rehabilitation
Your physiotherapist will guide you through the stages of rehabilitation including gait re-education, toe mobilisation exercises, swelling reduction and reducing muscle tightness. It is important to adhere to advice given.
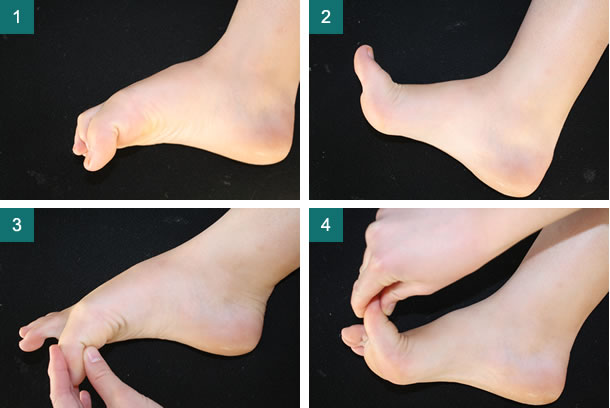
Cheilectomy movement exercises 1-4
When can I start to drive again?
DVLA states it is the responsibility of the driver to ensure they are always in control of the vehicle. A good guide is if you can stamp down hard with the foot to stop the car in an emergency stop. This will take at least 3 weeks. Click here to read DVLA guidance.
When can I work?
This is very individual and job-dependent. Below is a guide:
- Sedentary 2 weeks
- Manual labour 6 weeks
What long-term outcome can I expect after surgery?
Once the wound has healed you will gradually regain movement however it can take 3 months to be confident with your previous activities. It is a very successful operation with 90% patients satisfied. Mild swelling can persist in the foot for up to a year. The operation effect can last for years however depending on the severity of the initial condition, you may need further surgical intervention at some stage.
What are the risks?
Any operation carries a risk. Below is a guide to some risks potentially encountered. It is the surgeons duty to fully inform you of possible risks. Mr Roche will ensure this is always done so patients can make safe and informed choices about their operation.
Infection
If this happens, it is usually simply treated with antibiotics. Significant consequences from infection are very rare but can be dealt with. Risk is around 1%.
Nerve damage
Small nerves that supply sensation to the skin are near the incision site. Damage is rare but if your toe stays numb after surgery, the nerve may be bruised. If so it usually recovers. Risk is around 5%.
Deep Vein Thrombosis
Symptomatic clot formation in the leg is unusual after foot and ankle surgery (<3%). Whether treatment to prevent clot is needed can be discussed with your surgeon. There is no consensus amongst UK Orthopaedic surgeons as to whether preventative medicine is needed.
Important last note
This document is only meant to be a guideline to help you understand your treatment and what to expect. Every person is different and your rehabilitation may be quicker and slower. This will be advised and guided by your doctor and physiotherapist.


